Data Records and Clinical Coding
There are no software conformance requirements for this Requirement.
Practices must ensure that where clinically relevant, they are working towards recording the majority of diagnoses for active patients electronically, using a medical vocabulary that can be mapped against a nationally recognised disease classification or terminology system. Practices must provide a written policy to this effect to all GPs within the practice. An active patient is a patient who has attended the practice three or more times in the past two years.
Medical Vocabularies include SNOMED-CT, DOCLE, PYEFINCH and ICPC2+. Nationally recognised disease classification and terminology systems include ICPC2, ICD10-AM and SNOMED-CT.
Source: Practice Incentives Program eHealth Incentive guidelines—February 2013
DOCLE (Doctor Command Language) is a non-numeric health coding and medical classification system. The DOCLE system is used in Clinical.
DOCLE has been modelled on the Linnaean biological classification system since 1995. DOCLE generates clinical codes from ubiquitous health language using an algorithm, hence it is a human readable clinical coding system.
Preparing Your Patient Data in Clinical
Clinical Diagnosis Coder
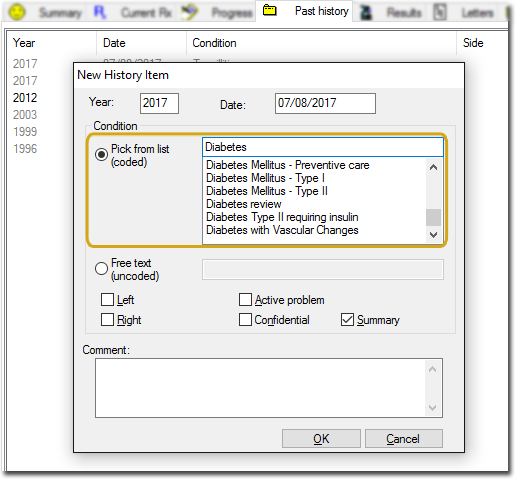
In MD3 there are two ways to enter past medical history items:
o Pick from list (Coded) or
o Free Text (Uncoded)
Both of these options are available to use in Past History. However if you have entered a diagnosis into the Past History tab that was not selected from the 'Pick from list' it will not be internally coded, and as such will not be found when doing searches. This is particularly important for Chronic Disease Management or when using some supplied decision support options.
For example, if you typed 'Diabetes type 2' into the uncoded section of the Past History tab, rather than using 'Diabetes Type II' from the drop down list, it will not be found when you do a search for Diabetic Type II patients.
How to Update Uncoded Past Medical History Items
MedicalDirector provides a simple utility in MedicalDirector Maintenance that enables you to easily find non-coded Past Medical History items, and either link them to a coded item or replace them with the correct coded item.
1. Double click the MedicalDirector Maintenance icon to open MedicalDirector Maintenance.
2. Select Clinical in the list of Database Tasks on the left of the window.
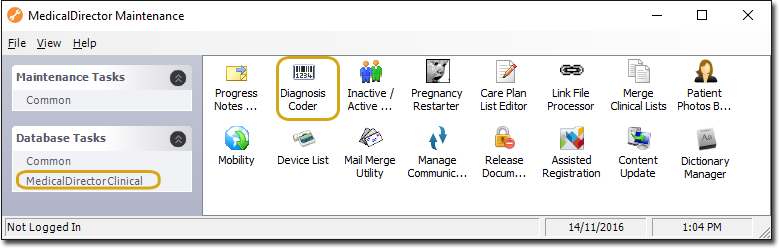
3. Double click the Diagnosis Coder icon. ![]()
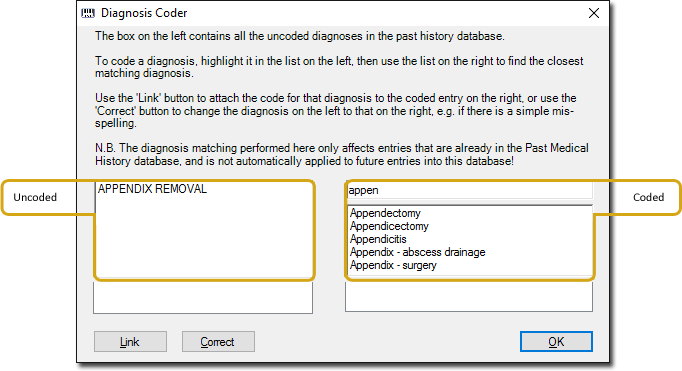
o The left-hand panel of this screen contains all the uncoded diagnosis entries in the Past Medical History database. The right-hand panel displays coded entries that you will select from to pair-up with your uncoded entries. Note that the right-hand panel is initially empty, but as you type into the text box above it (in this example appen), a list of items is generated underneath
o Simply highlight the entry on the left and the one you want to link or replace it with on the right, and then click either the Link or Correct button
o The  button will attach the code for that diagnosis to the coded entry on the right
button will attach the code for that diagnosis to the coded entry on the right
o The  button will change the diagnosis on the left to that on the right i.e. if the word was misspelled
button will change the diagnosis on the left to that on the right i.e. if the word was misspelled
o Once you have worked your way through all the uncoded diagnosis occurrences, all uncoded items will be replaced and coded, and therefore allow the now coded data to be included when conducting a search.
Important Resources
o NEHTA PIP implementation overview > Data Records and Clinical Coding
http://pip.NEHTA.gov.au/pip-implementation-overviews
o RACGP Standards for general practices (4th edition)
http://www.racgp.org.au/standards
o Australian Medicare Alliance – Data Quality Guide
http://www.amlalliance.com.au/__data/assets/pdf_file/0006/43971/Data-Quality-Guide.pdf