The “National Health (Pharmaceutical Benefits) Amendment Regulations 2019"4 and "The Veterans’ Affairs Pharmaceutical Benefits Amendment Instrument 2019"5 requires the inclusion of active ingredient name(s) on all RPBS/PBS prescriptions and allow for the identification of a brand if the prescriber deems this to be clinically appropriate for the treatment of their patient.
AIP is the second project under the Electronic Prescribing Initiative aims to increase the uptake of generic and biosimilar medicines. Many patients recognise their medication by the brand name, and there can be a risk of incorrect dosing if they take multiple medicines that contain the same active ingredient. Doctors will still be able to prescribe by Brand (noting the active ingredient must still be on the script) if the doctor considers this necessary for the medical treatment of the patient9.
Prescribing software are now required to comply by 1 February 2021.
1. Inclusion of the Brand as a default is prohibited under legislation
The regulatory amendments for AIP prohibit prescribing software from automatically including brand names on prescriptions by default, to ensure doctors make a clinical decision regarding the inclusion of the Brand.
The prescriber must make a clinical decision on the application of the brand name for every prescription.
2. Exemptions
The legislative amendments also enable the Secretary of the Department to determine some pharmaceutical benefits as exempt from active ingredient prescribing requirements. These items will be determined by the Department in consultation with the ACSQHC as described in the Guidelines for Active Ingredient Prescribing (See references to "LMBC" and "LEMI" in section 3).
3. Guidelines for Active Ingredient Prescribing
These guidelines will align with existing recommendations for medicines information display such as the Commission’s Recommendations for Terminology, Abbreviations and Symbols used in medicines documentation6 and the electronic display of active ingredient and brand name as described in the National Guidelines for On-Screen Display of Medicines Information7. It will also assist prescribers in making appropriate clinical decisions regarding the specification of the brand name following the active ingredient.
3.1 List of Medicines for Brand Consideration – (LMBC)
This list identifies medicines for which prescribers should consider if the inclusion of the brand name on the prescription is necessary for their patient.
The presence of a drug on the RLDBI is intended as a guide only. It is not used as an absolute dictum which prescribers must follow noting that the inclusion of the brand name may apply to any drug and will be driven by the prescriber implementing a decision based upon the appropriate clinical outcome for the patient.
Considerations for prescribing RLDBI Drugs
Where an RLDBI item has been selected:
o and the prescriber has NOT intentionally nominated a brand
o and the prescriber has not been previously prompted during this prescribing event to consider including a brand, the software may prompt the prescriber to consider if the inclusion of the brand name on the prescription is necessary for the clinical treatment of their patient.
i. Prescriber selects the drug by Active Ingredient:
As a specific brand has NOT been selected, the active ingredient name(s) only would normally be included on the prescription. However, if the medicine is on the LMBC, the prescribing software can prompt the prescriber "to consider" if the inclusion of the brand is clinically appropriate for their patient.
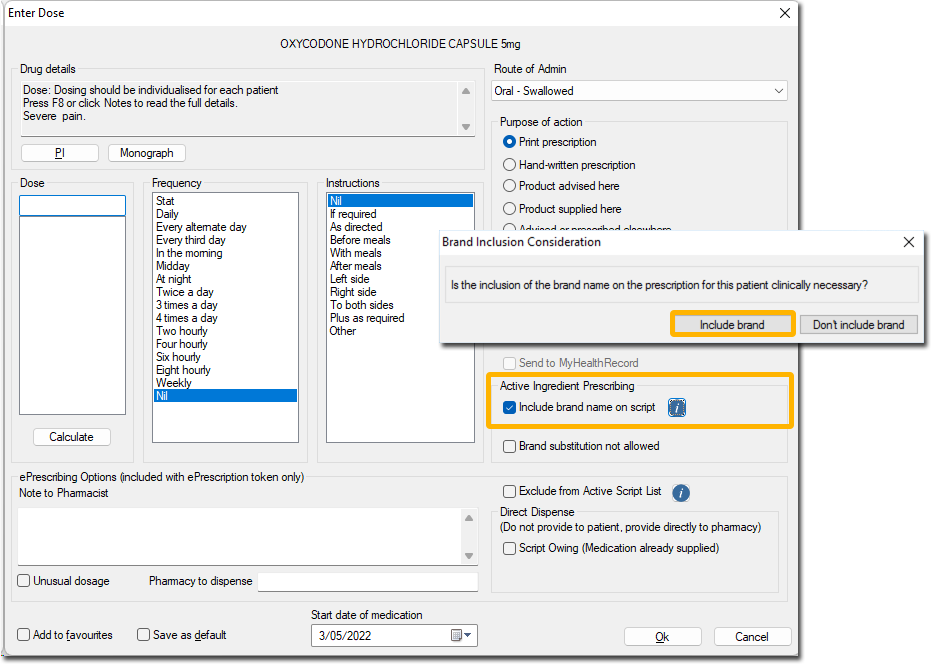
Figure: MD Clinical prompting for brand inclusion consideration
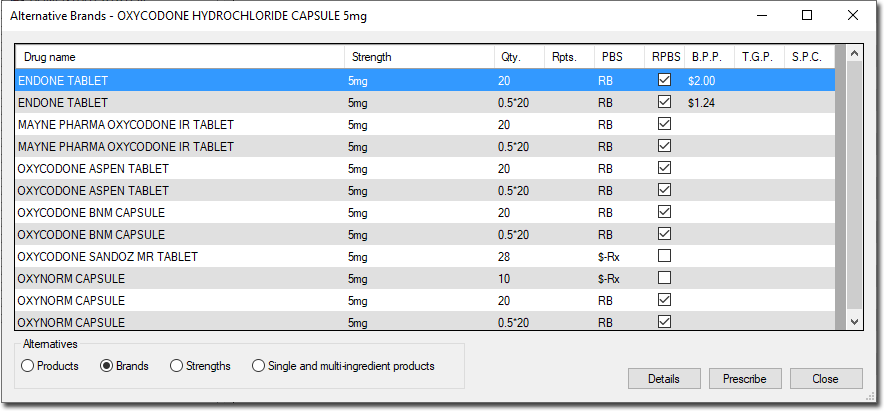
Figure: Alternate Brands window appears if user selects to include brand name
ii. Prescriber selects the drug by the brand:
The prescription must still include the active ingredient name before the brand except for the LEMI items.
In MedicalDirector Clinical, ‘Include brand name on script’ is ticked by default for all LMBC drugs. The prescriber is displayed with the brands available for the selection. On printing such medication, the active ingredient appears first followed by the brand name in the bracket.
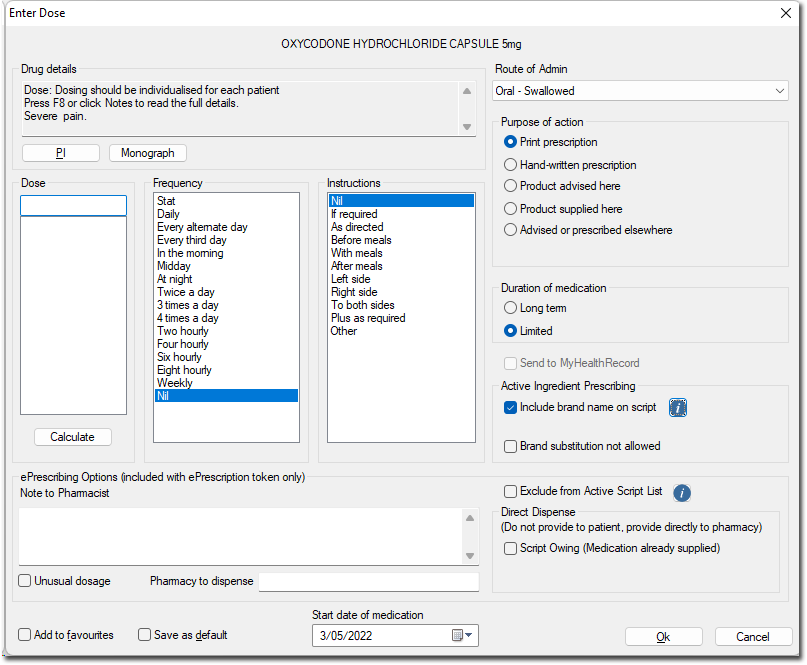
Figure: ‘Include brand name on script’ is enabled by default for LMBC drug
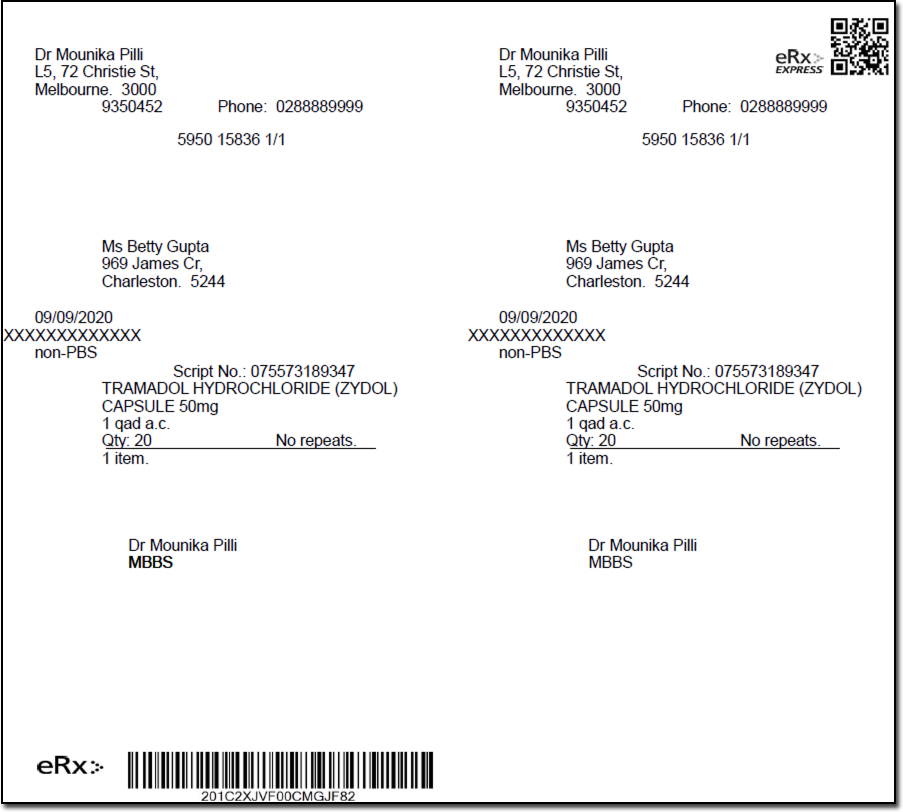
Figure: The active ingredient(s) must appear first when the brand name is included
3.2 List of Excluded Medicinal Items (LEMI)
The LEMI identifies drugs which are excluded under the AIP legislation from the mandated requirement to include the active ingredient names(s) on the prescription and which therefore may be prescribed by the brand name only.
Figure: ‘Included brand name on script’ option is enabled by default for LEMI
Figure: Script with brand name only
As these drugs are specifically nominated by the legislation or identifiable by the classes, general terminology or the scenarios under which their prescribing occurs, the LEMI drugs are not subject to individual MPP identification via an AMT reference set.
4. Situations excluded under the AIP Legislations (LEMI)
This section describes the medicines and prescribing events which are excluded under the Active Ingredient Prescribing Legislations where the active ingredient name(s) are NOT mandated thereby allowing the medicinal item to be prescribed by the brand name only.
o Handwritten prescriptions.
o Prescriptions with four or more active ingredients9
o Items listed under the "VARIOUS" section of the General PBS Schedule including:
• Allergens
• Diagnostic Agents
• General Nutrients, Food Supplements, Vitamin Supplements o Wound Assessment and Dressing Section
o DVA has included Items listed under the "VARIOUS" section of the RPBS Schedule including:
• Allergens
• Diagnostic Agents
• General Nutrients, Food Supplements, Vitamin Supplements
• Other Non-Therapeutic Products
• Wound Assessment and Dressing Section
o Computer generated paper based National Residential Medication Charts.
o Prescriptions generated by a prescriber through a free text function within prescribing software as detailed in paragraph 6.1.
o These requirements do not apply where it would contravene State or Territory legislation.
5. Re-Prescribe or Duplicate Script Functions
This is another common facility provided by some prescribing software systems, whereby the prescriber accesses the patient history and selects a script in the history to create a new prescription identical to the one selected.
It is important to ensure that the re-prescribed item must follow the current AIP rules and not the rules as saved when previously prescribed.
6. References
1. http://www.tga.gov.au/industry/artg.htm
3. https://www1.health.gov.au/internet/budget/publishing.nsf/Content/budget2018- factsheet13.htm
4. https://www.legislation.gov.au/Details/F2019L01312
5. https://www.legislation.gov.au/Details/F2019L01387
6. https://www.safetyandquality.gov.au/publications-and-resources/resource-library/recommendations-terminology-abbreviations-and-symbols-used-medicines-documentation
7. https://www.safetyandquality.gov.au/publications-and-resources/resource-library/national-guidelines-screen-display-medicines-information
8. https://dev.pbs.gov.au/embargo/index.html
9. https://ama.com.au/ausmed/changes-way-you-prescribe-%E2%80%93-electronic-and-active-ingredient-prescribing
10. https://www.humanservices.gov.au/organisations/health-professionals/topics/education-guide-prescribing-dispensing-and-claiming-hsd/32081
11. https://www.tga.gov.au/accessing-unapproved-products
12. https://www.tga.gov.au/form/special-access-scheme
13. https://www.tga.gov.au/access-medicinal-cannabis-products-using-access-schemes